Last week, the federal government announced the distribution of the first $30 billion in funding for hospitals via the United States (US) Department of Health and Human Services (HHS) Public Health and Social Services Emergency Fund (PHSSEF). The funding can be used to support healthcare related expenses, lost revenue attributable to the novel coronavirus (COVID-19), and to guarantee uninsured Americans have access to testing and treatment.
The first tranche of this HHS funding is based on historical Medicare fee-for-service revenues and began arriving as direct deposits to hospitals this week. Initially, the fund was to be based on rolling applications, but the government opted for an immediate infusion into the healthcare system. These are payments — not loans — and hospitals will not need to repay these funds.
While the funding is intended to help hospitals, it may disadvantage those with the greatest need. The first allocation was based on revenue from the Medicare program, not COVID-19 burden or unmet need. Essential healthcare systems that are hard hit and rely on Medicaid or private payers for survival are not seeing relief from the first tranche. The current methodology ignores large urban hospitals on the frontlines of battling the coronavirus and may be treating a disproportionately high rate of uninsured patients. Funding delays to these hospitals jeopardizes their financial viability.
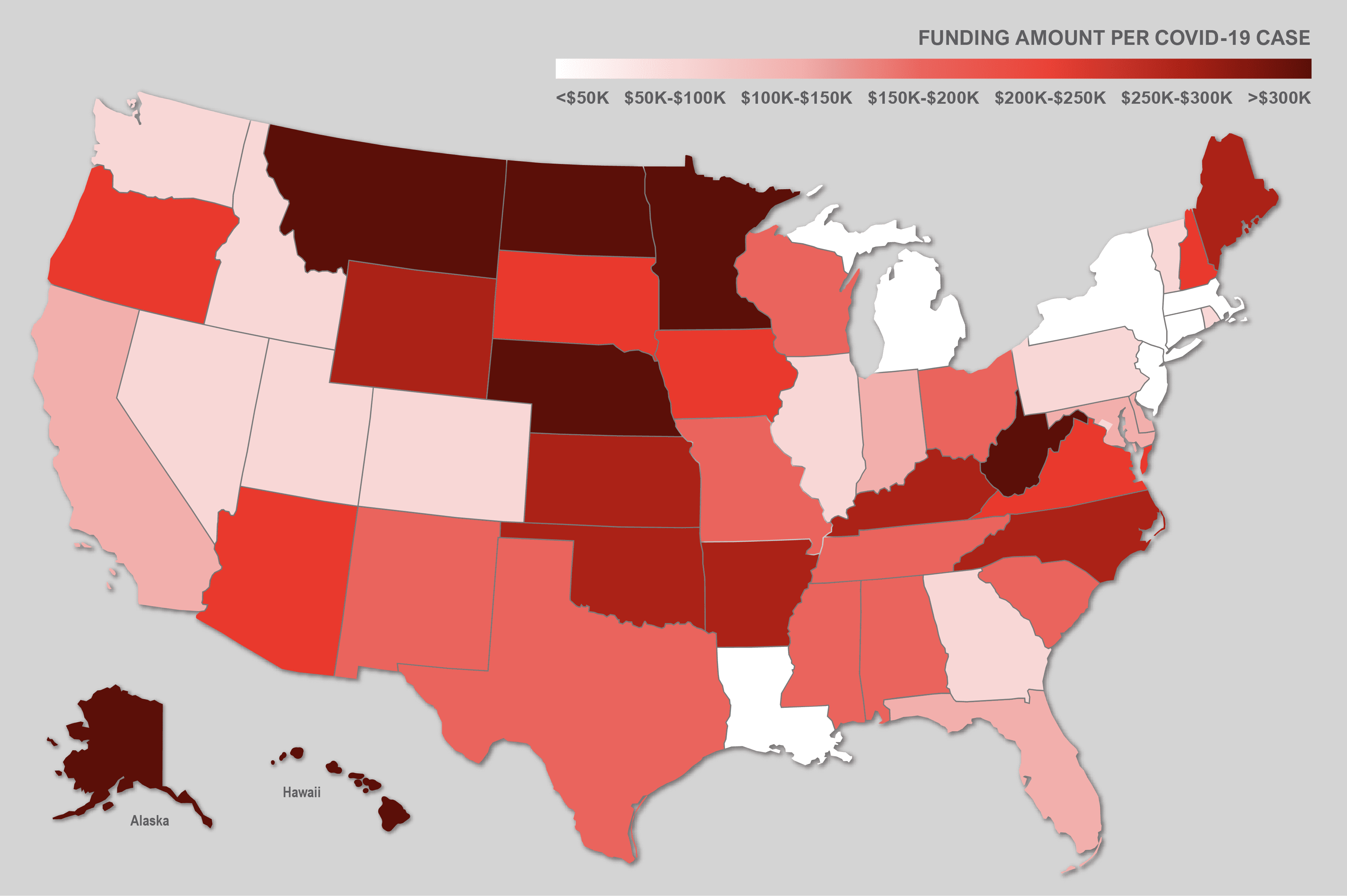
An analysis of the first $30 billion shows hospitals in states such as New York and New Jersey, which make up the majority of COVID-19 patients, are receiving $12,000 and $18,000 per case, respectively. In contrast, states with far fewer cases — Hawaii and Wyoming — are receiving $301,000 and $278,000 per case. In total, hospitals in the Commonwealth of Massachusetts are receiving approximately $1.2 billion with more than 25,000 cases, while hospitals in North Carolina are receiving approximately $1.3 billion for their 5,000 cases. The map below illustrates the amount of PHSSEF distribution per COVID-19 case by state.
For hospitals that received funds, they must sign and submit an attestation to HHS within 30 days confirming receipt of the payment and agreeing to the terms and conditions. If a hospital does not want to comply with the terms and conditions, there will be a process to return the funds to HHS. The attestation portal is open and can be found online.
The key limitations include the following:
- The payment can only be used to prevent, prepare for, and respond to coronavirus, and shall reimburse the recipient only for healthcare-related expenses or lost revenue attributable to COVID-19.
- The recipient will not use the payment to reimburse expenses or losses that have been reimbursed from other source or that other sources are obligated to reimburse.
- Hospitals are banned from surprise (balance) billing out-of-network COVID-19 patients including those with a possible case of COVID-19.
In addition, HHS is imposing quarterly reporting requirements on recipients that receive more than $150,000. Recipients will need to carefully track their expenses and revenue losses and will need to comply with the HHS’s reporting and record retention requirements.
As of today, it is not clear what the remaining $70 billion will fund or how it will be allocated. The subsequent round of funding, anticipated in a few weeks, may target non-Medicare providers (children’s hospitals, nursing homes, pediatricians), COVID-19 hot spots, and rural providers. Despite the fund’s shortcomings, the HHS emergency fund is one of the only funding streams focused on hospital and healthcare lost revenue. PHSSEF highlights the need for additional federal legislative packages further addressing a loss revenue and the need for better financial metrics to assess hospitals and healthcare providers overwhelmed by COVID-19.

For hospitals and healthcare systems seeking to leverage the COVID-19 federal funding opportunities, Hagerty can provide expert advice and assist your organization with short-term liquidity and long-term recovery funding guidance. To learn more about COVID-19 recovery funding opportunities and to learn more about Hagerty’s cost recovery practice, visit our Recovery Page.
Amelia Muccio is the Director of Mitigation at Hagerty Consulting and a subject matter expert in recovery and healthcare systems. With over 20 years of experience in public health, disaster preparedness, mitigation, and financial recovery, Amelia has helped clients obtain $5B in federal funds after major disasters, including Hurricane Sandy, the California Wildfires, and Hurricane Harvey. In addition, she worked as the director of emergency management for the New Jersey Primary Care Association, where she specialized in integrating community-based health centers into statewide planning and response efforts for bioterrorism and large-scale emergencies. She managed the Tamiflu distribution to community health centers during the H1N1 pandemic and has trained more than 5,000 healthcare professionals in Incident Command System, National Incident Management System, and the National Response Framework.